May serenity, wisdom and kindness find us all this year and may abundant health become the given, the benchmark, that allows for freedom & ease each and every day for all of us.
Comforting, unassuming, highly satisfying black eyed peas served with coconut rice :: the perfect start-on-the-right-foot New Year’s meal.
It’s apparently an old southern US tradition to eat BEPs on New Year’s day as a call for good fortune and abundance. Not a thing we usually do in Québec but hey!, never too late to add in a new wholesome tradition to the roster.
This humble legume’s story is said to date back to more than 500AD Rosh Hashana; it has “traditional celebration fare” status during the Jewish holiday. Or so I read…
It’s combination withrice is said to have been brought to our side of the pond by West Africans who, through the somber story of their arrival in American soil, managed to hold on to this simple, grounding and nurturing tradition.
That being said, a meal is a meal is a meal; it’s supposed ability to bring about “good luck” shall be judged by the person making and eating it! 😉 I eat it ’cause it’s delish :: if a little more goodness comes my way with a few fuss free spoonfuls, you can bet I’ll take it.
What I do know for sure though is that legumes are the most underrated food in the “Shiny Health & Wellness” online world. They’re not sexy, I’ll give you that!
Being extremely inexpensive makes them somewhat less “luxurious and covetable” than that 15$ a serving bright pink, dragonfruit-and-all-the-superfoods utterly instagramable smoothie bowl! I’m sure you’ll agree though, a bean dish is more real life and acceptable for most families out there…
They are most definitely usually associated with simpler, “old-style peasant family” times and there is something quite charming about that for me…
In my book, they are ALSO associated with ::
*For a 1 cup cooked serving
Half your day’s fiberrequirements :: the grand (and also underrated!?) gift of regularity and practically free microbiome food/ prebiotics.
Half your day’s copper requirements :: useful in iron transport and energy production.
An impressive 85-90% of all the folate you need in a day :: essential to proper cell division and DNA synthesis. *Any pregnant/ trying to conceive ladies in da house!? Dietary folate should rank high on your priority list.
13g of super well-balanced protein building amino acids and an especially rich source of essential phenylalanine, a dopamine precursor :: think motivation, satisfaction and pleasuuurree!
Combined with brown rice, spinach and a few more basic veg kitchen staples; you get medicine that most definitely doesn’t require a teaspoon of sugar to help it go down.
Make it, any day of the year, to bring a little more health, and mayyybe some good fortune, about…
Stay curious and humble!
A truly happy New Year to you,
Vicky x
Thyme Scented Black Eyed Peas over Coconut Spinach Rice
Ingredients – BEPs
1 tbsp neutral, high smoke point oil such as avocado
*or water sauté if avoiding oil
2 large stalks of celery, finely diced
1 large yellow onion, finely diced
1 large carrot, finely chopped
1 medium parsnip, peeled and finely chopped
*Could be scrubbed instead of peeled is skin is fresh and thin.
2 garlic cloves, minced
2 bay leaves
1 big yellow potato, scrubbed and diced in ½” pieces
1 ¼ cup dried black eyed peas, soaked in water overnight, water discarded and thoroughly rinsed and drained
3 cup unsalted/ low salt veg stock
1 red chili of your choice, split lengthwise
1 tbsp dried thyme
S&P, to taste
Method
In a heavy bottom pot on medium heat, sauté celery, onion, carrot and parsnip until lightly golden. About 10 minutes. Add in garlic, bay leaves, thyme and chili. Cook for an extra 3-4 minutes. Add in a touch of boiling water if things seem to want to start sticking.
Add stock, beans and potato and bring to boil on high heat.
Bring the temperature down to simmer, cover, and cook 90min.
Ingredients – Rice
1 tsp neutral, high smoke point oil such as avocado
*Or water sauté if avoiding oil
1 large yellow onion, diced
4 strips tempeh bacon
*or Paradis Végétarien Vegan Bacon, if available to you.
1 cup brown basmati
1 can full fat coconut milk
If you are on a journey where saturated fats are being limited, go for light milk!
100ml water or unsalted/ low salt vegetable stock
3 “nuggets” (85g) frozen spinach
S&P to taste, keeping in mind the veg bacon is salty
Method
In a saucepan on medium heat, sauté onion and tempeh/ veg bacon in a tsp of oil until golden brown.
Add in the rice, mix well and toast for 2-3 minutes, stirring frequently.
Add in coconut milk and water/ stock and bring to a boil.
Reduce heat to med-low or low to simmer, covered, for 20-25minutes.
When rice is almost cooked, add in the frozen spinach nuggets on top of the rice and put the lid back on for 3-4 minutes until mostly thawed.
Mix well, adjust seasoning to taste.
Serve topped with beans and their broth and top with thai basil// mint// basil, minced chilis, a lil’ more crispy vegan bacon, green onions…
Combine with a super simple green salad with tomato, refreshing cucumber and copious amounts of lemon juice to “cut” through the richness of the coconut fat and you have yourself a well-balanced, ultra-satisfying meal.
Enjoy!
Whole recipe nutritional info broken down for 5 servings (side salad not included) :: 560kcal as 55% whole food carbs, 32% fat and 12.5% protein. 15g of fiber, 19g of protein, 6mg of iron, 940mg of potassium, 2mg zinc and a rich source of B1, B6, vitamin A, C, K, copper, magnesium, manganese…
*Inspiration Rodger Mooking on Marylin Dennis Show “Lipsmacking Chicken Rice”
Many, but not all, things one must know about iron are on this page :: how much you need, iron depletion causes, effects of inadequate dietary intake, dangers of over supplementating and little tricks to optimize absorption.
Health Canada’s DRIs – Dietary Reference Intakes suggest daily intakes of ::
Male, adults and children :: 8mg/ day EXCEPT for teenagers aged 14-18 where needs creep up to 11mg/day
Female, age dependant :: 9-13 years of age need 8mg/day just like all women older than 51.
Teenage girls (14-18) :: 15mg/day
Menstruating adult women (19-50) require 18mg/day.
Pregnancy :: needs shoot up to 27mg/day. *Lactating :: 9mg/day
Upper limit sits at 45mg/day for all (children 40mg).
Any dose higher than these reference values should be evaluated by a health care professional.
There! These are the numbers that should cover the needs of the majority of healthy individuals.
These suggested values represent a sufficient amount for most but not necessarily anoptimal one for all. Individualising these suggestions should be considered, but in order to do that, I’m afraid you’ll have to keep reading and/or meet up with a health professional who can assess your needs and save you the reading. 😉
Iron is a mineral the body cannot produce and needs for growth, repair and function.
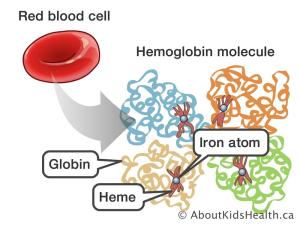
It is a crucial component of hemoglobin (and myoglobin), a component of red blood cells which carries oxygen through the body. It’s also used in “energy making” processes.
It is essential to the assembly of numerous enzymes and the stabilization of certain proteins. (via Iron-sulfur clusters). *Enzymes are VITAL for our biochemistry to actually… work.
As a constituent of cytochrome P-450 superfamily of enzymes, it works hard to maintain “body balance” by breaking down xenobiotics (think pollution, plastics and perfumes), fatty acids and various compounds. CYP450 is very much involved in several hormones’ production and clearance. Production of TSH and thyroid hormone T4’s conversion into T3 are 2 examples. It plays a role in adrenal function regulation (think stress and alertness), insulin metabolism (think steady energy), sex hormone regulation (conversion of androgens to oestrogens), DNA damage recognition and repair 1, 2, 3, 4 …
Iron levels may also play a role in regulating “leptin” hormone. Anemic individuals frequently suffer from low iron induced appetite loss. In these people, iron supplementation, or sufficient dietary intake of the nutrient, has an inhibiting effect on the satiety hormone leptin. This leptin inhibiting phenomenon increases appetite so the individual has a desire to tap into (and benefit from!) the perceived abundant available iron source” 5 .
Iron comes in 2 forms ::
Fe2+, Ferrous // HEME iron :: mostly animal based
Fe3+, Ferric // NON-HEME iron :: plant based
Absorption mechanisms of these 2 forms of iron are discussed here ::
In a nutshell :: animal/ muscle based iron is less abundant yet more easily absorbed than its plant based counterpart which is omnipresent but not as fully absorbed.
Iron intake and supplementation should be tackled with a prudent approach as iron is both essential to the body’s wellbeing and deleterious when consumed in excess.
Oversaturation of iron triggers the production of free radicals that cause premature and accelerated cell aging. A great image to keep in mind is “iron that rusts”. While not 100% accurate, I find this analogy to be a great reminder of what can happen to our cells when iron regulation goes awry and the mineral starts to “build up & act up”.
Main sources
Sources of Animal based iron ::
Beef (sirloin) :: 100 g – 2.9mg *See also liver
Oysters (raw) :: 100 – 5.1mg *See also cuttlefish, octopus and mussels
Tuna (canned) :: 100g – 1.5mg *See also sardines
Chicken (breast, skinless) :: 100g – 1.1mg
Pork (ground, cooked) :: 100g – 1.3mg
Sources of plant based iron ::
Dried apricots :: 100g – 2.7mg *See also prunes, figs and raisins
Lentils :: 100g – 3.3mg *See ALL beans and tofu/ tempeh
Spinach (raw) :: 100g – 2.7mg *See also swiss chard and broccoli
Oat flakes (dry, whole grain) :: 100g – 4mg *See also quinoa and barley
Oyster mushrooms (raw) :: 100g – 1.3mg
Pumpkin seeds :: 100g – 8.1mg *See also sesame seeds
**Some products like cereals, noodles, breads and bagels, while not usually significant sources of iron, are now enriched with supplemental iron.
A healthy body is absolutely capable of regulating the uptake of iron as it needs it; dietary overdose is extremely rare in most.
Overdosing is possible with supplementation which is why nutrition correction and optimization should always be your “go-to”.
Excess iron intake has been linked to increased oxidative stress.
Evaluating iron needs
Vegetarian consumption of “beans & greens” in the daily diet 6:: not a fan of either? These 2 rich whole food sources of iron don’t find their way into your plate daily? It would be wise to have your levels checked.
Individuals who eat a nutrient poor diet consisting of “pseudo/ non-food foods” might not be meeting their needs.
Pregnancy ups a woman’s iron needs by 9mg :: Are you aware of your daily intakes? Could you come up with a dietary combo representing those 9 extra mg? If not, naturopathic guidance could definitely be useful.
Menstruation :: there is an assessment to be made here. Light? Short? Long? Heavy? Any combination of these 4 factors will impact your needs in different proportions.
High level athletes’ iron losses are always considered a little higher (hemolysis, excessive sweating) *Fitness enthusiasts do NOT worry, the greatest majority of us are NOT considered high level athletes. Chill. 😉
Chronic bleeding induced by various pathologies :: stomach ulcers, intestinal polyps, colon cancer, celiac disease… Endometriosis could also cause bleeding one might not be aware of. Any type of recurrent bleeding makes the needs go up.
Frequent aspirin ingestion; notoriously hard on the stomach mucosa, it could trigger bleeding you might not be aware of.
Gastric bypass surgery :: the digestive process is no longer complete nor optimal. Having your levels and needs assessed frequently by a medical doctor is mandatory. A naturopath can most definitely help you optimise your new physiology.
Infectious and inflammatory conditions (including obesity) also play important roles in determining needs, which might be a tad higher than most 7
Optimising absorption
Black pepper is one of those substances that are wiiidely known as “potentiators of absorption“. Some studies correlate Bioperine*/ piperine with better iron absorption 8.
*Bioperine is a trade name of a specific brand of black pepper extract.
Algae consumption might also be a wise move if better iron absorption is on your mind :: “the bioavailability of this iron (algal) seemed to be high, and increased apparent iron absorption up to 5-fold of the absorption value of the rice meal alone. This was probably due to the high vitamin C concentration and also to the low or nonexistent phytate content. 9”
Although there are PLENTY of whole food sources available to us now, we sadly don’t often consume algae in North America. Chopped sea bacon (dulse) is a great umami/ savoury salad topper, a little handful of rehydrated wakame in a noodle dish, classic nori sheet wrapped around room temp brown rice and avocado; there are countless ways sea veggies can “sneak” their way into our daily diet.
Should supplementation be suggested after a professional assessment, ingestion of the chosen supplement should be done every other day to maximise absorption.
Here’s why ::
As iron rolls in, its absorption triggers the release of the hormone that’s responsible for regulating its intake (hepcidin). In short :: when iron is abundant, hepcidin RISES and sloooows its absorption (It prevents overload).
A study from 2020 (19 women) suggests that skipping a day in between supplement doses gives time for hepcidin to “back down” and stop hindering the absorption process. Read :: it benefits iron’s uptake! This simple trick can make your hard earned dollars go further and your intended “iron level UP efforts” more efficient 10, 11, 12.
Vitamin C is also a classic cofactor of iron metabolism, it aids in plant based iron absorption 13.
Important players in the Iron game
B6 – Pyridoxine :: This water soluble vitamin is needed for red blood cell formation (erythropoiesis). It plays a pivotal role in the incorporation of iron in the heme of HEMoglobin (protoporphyrine). Sub-optimal intake of this vitamin is linked to a higher incidence of anemia and many other health problems 15, 16.
B9 – Folate :: also works with iron (and B6 and 12!) in the red blood cell formation process. One without the other(s) is the equivalent of trying to travel without a passport and a suitcase. High alcohol consumption, celiac disease and IBS could all increase your personal requirements of this particular nutrient 17, 18, 19.
B12 – Cobalamine :: This vitamin plays an important role in cell proliferation. As red blood cells have a lifespan of approximately 120 days, their replacement is constant. They do not only require B6 and B9 to form properly but also B12 to ensure proper growth. A B12 deficient red blood cell is an inefficient one that simply cannot make it and dies. While cobalamine might not impact iron absorption directly, it does so indirectly by keeping iron rich hemoglobin INSIDE healthy blood cells thus preventing an endless need for iron recycling and replenishing the body tirelessly tries to accommodate A.
Copper :: This mineral is needed for iron “transport & dispatch”. Just like iron, a “Goldilocks” approach is best when optimising copper levels :: not too little, not too much as both ends of the spectrum can have deleterious effects on wellbeing 20, 21. Supplementation without the advice of a health care professional is not suggested. Dietary sources of copper are :: liver, dark chocolate, oysters, leafy greens, spirulina, nuts & seeds and shiitake mushrooms. If you wish to understand how copper participates in iron metabolism, read the article on the topic showcased further up.
Precautions
The most common concerns with steady iron supplementation is gastrointestinal disturbances.
Again :: one MORE good reason to prioritize dietary sources over supplementation, if you can. Gastric discomfort, nausea, vomiting, constipation and diarrhea are the usual culprits.
Alternate day supplementation, as suggested above for better absorption, might reduce the risk of uncomfortable manifestations and actually enhance your adherence to a supplementation protocol.
Exaggerated intakes
Breast cancer and iron :: a diet that is LOW in antioxidant and overabundant in both fats and iron may play a role in increased breast cancer incidence (via lipid peroxidation) 22.
Myocardial infarction and iron :: Overconsumption of HEME iron, the animal based kind, coupled with a diet that is low in minerals responsible for slowing iron absorption can lead to cardiovascular issues23.
Type 2 diabetes and iron :: again, overconsumption of HEME iron, the animal based kind, can lead to an increased risk of developing type 2 diabetes 24.
Colorectal cancer and iron ::one more time, altogether :: OVER consumption and/or a poorly elaborated iron supplementation protocol can lead to an increased risk of developing colorectal cancer 25.
Sub-optimal intakes and associated risks
You’ll have to read the piece on anemia that is coming shortly, it’ll explain all the discomforts low iron can trigger.
In the meantime, get acquainted with these classic symptoms of low iron and see where you land.
Intense fatigue // Tired even after resting
Shortness of breath
Sore tongue
Irregular heartbeats
Weakness
Chest pain
Dizziness // Light headedness
Cold extremities (hands and feet)
Brittle nails
Pale skin
Headaches
Factors that should have you pay attention to your iron levels
If you are taking Proton Pump Inhibitors, such as omeprazole, for gastroesophageal distress and/or to prevent stomach ulcers caused by regular intake of aspirin or other NSAIDs/non-steroidal anti-inflammatory drugs; you might be at higher risk of inadequate iron intake 26.
Important and steady ingestion of quercetin supplements are suspected to up levels of hepcidin (which DECREASES iron uptake) while also diminishing the number of available plant iron transporters in the intestine resulting in less iron uptake (DMT1). Quercetin supplementation is, among other things, often suggested for allergy support.
*On the other side of the spectrum, should you be in a situation of iron overload, quercetin might be something you want to discuss with your health care professional, as a method of minimizing further iron absorption 27.
Do you crave non-food/ non-nutritive things like, dirt, ice, rubber or clay? We call this condition Pica, and it could be an indicator of inadequate iron stores 29.
Do you suffer from sudden/ unexplained hair loss? While it is still not clear exactly through what mechanism low iron impacts hair growth and retention; it is widely accepted as one-more-sign that can be correlated to other low iron contributing factors 30, 31 .
Restless leg syndrome a bit like hair loss, while poorly explained, presents a very strong correlation to inadequate iron levels32, 33.
Behavioral and/or learning deficits, especially in childhood and adolescence. Some would describe it as “resembling ADHD”. This one is quite vague and MUST definitely be assessed by a professional; one’s perceived deficits being a solid indicator that a discussion should be had. A million things can influence behavior and cognition, iron just so happens to be one of them 34.
Always remember :: No isolated “sign or symptom” represents inadequate levels in itself; all factors should be put together and assessed with a multifactorial mindset .
Blood tests
*Blood tests are prescribed and interpreted by medical doctors. Iron values can be included in blood tests, all you have to do is ask.
Reference values :: they differ for men and women and are quite numerous when evaluating the full picture; here is a link to medically approved values for those of you that are curious.
As with most things related to health, one blood value is not enough to evaluate needs and/ or actual state of vitality; other aspects must be investigated to round out the results.
A few precisions on inhibiting combos
Avoid these foods 2hrs before and after a therapeutic dose/ intentionally iron rich meal 35, 36 ::
Polyphenol/ tannin rich foods such as tea, coffee, wine and dark chocolate which have a “tightening effect” on the mucosa and can make absorption of some nutrients, not just iron, a little more difficult. *Tannin rich foods’ effects are dose dependent; the more you consume, the more they inhibit iron absorption. Minimal intakes can be mitigated by the regular addition of vitamin C to the diet 37.
Phytate containing foods such as raw grains, beans and nuts & seeds. It’s important to keep in mind that phytates are a “dose dependent inhibitor” too and that cooking, fermenting, sprouting and soaking all contribute to lowering the phytate content of these foods making them a negligeable sources of phytate in their actual prepared edible forms. (*Common misunderstanding :: Oxalic acids / Oxalates are NOT related to phytates. They are a different beast :: they do NOT hinder iron absorption)
Calcium rich foods have been thought to hinder iron absorption in the past but now, the correlation isn’t so strong. If you ARE supplementing, it could be beneficial to avoid taking both minerals at the same time, but as whole food items; I wouldn’t sweat it as the inhibitory effect is usually short lived and actually compensated by an increase in iron transporters/ “absorbers” a few hours later.
Egg proteins have an inhibitory effect on iron absorption AND the iron they contain is of poor bioavailability once cooked (Hard boiled eggs :: when that yolk turns a little green/gray?! Iron sulfide :: no longer absorbable.).
Antibiotics and other medications :: Iron supplements can go both ways :: they may decrease the absorption of certain medication, making them LESS effective. And certain drugs can also boost iron absorption and storage to concerning levels. The “2hrs before, 2hrs after rule” is quite important here (unless specified otherwise by your medical doctor). A few interactions are listed in this article.
Controversial Turmeric :: while some studies show it may stimulate iron uptake through a decrease in hepcidin expression OTHERS give it “chelating” properties which have the power to bind to iron and actually prevent its absorption. Individual assessment is of course needed and wise in this particular case.
ALSO :: If you are on a supplement regimen, avoid consuming fortified foods to limit possible “over ingesting” the mineral.
There you have it, a little cheat sheet on iron!
A few studies have been linked throughout this article; get acquainted with the data if you wish to know more about this topic. This post is merely a quick and simplified intro into the subject.
Research papers are always a great way to approach a discussion with your health care provider, feel free to share them with yours if you think it would be useful in the evaluation of your specific needs and the enhancement of your vitality.
Stay curious and humble,
Be well,
Vicky x
Vicky Bachand ND.A is a naturopath :: a naturopath does NOT replace a medical doctor.
Ideas provided in this article are presented as information only and do not aim to provide in depth details about the chosen topic nor replace the advice of a qualified health care provider.
Information shared here does not constitute a consultation, a diagnosis nor a medical opinion and therefore should not be interpreted as such.
Always consult with your chosen health care provider if you have questions about your personal health.
Si vous ne retenez qu’une chose de cet article, que ce soit celle-ci ::
Le fer est à la fois ESSENTIEL et TOXIQUE pour l’organisme humain.
Dans notre société où plusieurs semblent adopter l’adage :: « Si UN PEU c’est bien, alors PLUS est inévitablement mieux » je souhaite mettre une emphase particulière sur le fait que cette mentalité s’applique très peu aux processus métaboliques humains.
Le corps étant conçu pour, inlassablement, dissiper les excès et pallier les carences que nos modes de vie lui imposent; pourquoi vouloir le surcharger à outrance?
La supplémentation en fer isolé doit se faire « À la Boucle d’or »; elle est fortement déconseillée sans la supervision d’un professionnel de santé.
Notoirement difficile à absorber, le fer est également très difficile à éliminer et met tout individu y allant « à tâtons » dans le merveilleux monde de la supplémentation à risque de surcharge.
Le fer a plusieurs rôles dans le corps humain ::
Transport d’oxygène
Transfert d’électrons
Respiration cellulaire –> création d’énergie!
Synthèse et réparation d’ADN et protéines
Synthèse de l’ARN
Cofacteur de nombreuses enzymes :: enzymes qui sont essentielles à TOUTES les réactions biochimiques du corps humain.
Participe à la formation des hémoprotéines :: hémoglobine, myoglobine, cytochromes…
En excès et/ou en cas de régulation compromise, il entrave le bien-être humain ::
Il peut être promoteur de formation d’espèces réactives de l’oxygène (ROS/ FRO) qui peuvent causer des dommages à l’ADN et/ou inactiver certains enzymes. En termes simples, on pense :: radicaux libres toxiques. Le fer mal régulé/ excédentaire a la capacité de provoquer un vieillissement accéléré des cellules. (Réaction de Fenton)
Cette mise en garde bien établie, voyons comment le corps humain régule ses apports et ses stocks de fer.
Apports
Le fer est d’abord dit « essentiel » parce que le corps ne peut le synthétiser et donc, des sources alimentaires doivent impérativement être consommées.
Les apports se présentent sous 2 formes ::
**Notion à laquelle les végé voudront porter une attention toute particulière :: l’absorption de ces 2 formes de fer ne se fait ni pareillement, ni également.
Fer ferreux/ Fe2+/ fer héminique :: Environ 10% du fer alimentaire, il représente approximativement 1/3 du fer absorbé. On parle de fer de provenance animale intégré à des molécules d’hémoglobine et de myoglobine analogues aux nôtres. “Héminique” traduit la présence d’héme, le fer y est logé. On pourrait comparer ce type, si on utilise une analogie un peu douteuse, à un baigneur (le fer) arrivant à la piscine avec un manteau (l’hème) par-dessus son maillot d’bain. Stick with me! J’promet que ça va être utile plus bas. 😉
Fer ferrique/ Fe3+/ fer non héminique/ Inorganique :: Environ 90% du fer alimentaire, il représente approximativement 2/3 du fer absorbé. Ce fer végétal est libre d’hème; il est un peu comme un baigneur qui arrive à la piscine publique nu comme un ver :: sans manteau, ni maillot. Vous comprendrez donc que certaines modifications devront être faite avant de le laisser entrer celui-là.
Absorption de fer Fe3+/ NON Héminique dit inorganique
Dans le tube intestinal, le fer ferrique de source végétale, Fe3+, ne peut être absorbé; une enzyme doit d’abord altérer sa charge (le DCYTB, majoritairement). Cette enzyme a besoin pour opérer de vitamine C. Si vous avez déjà entendu ou lu qu’il est avantageux de coupler ses apports de fer végétal d’une source de vitamine C :: c’est pour cette raison!
PAS de vitamine C, pas d’altération possible de la molécule de fer = PAS d’absorption.
L’analogie douteuse est de retour :: il en revient à demander à notre baigneur nu de bien vouloir mettre un maillot avant d’entrer à la piscine. L’entrée requiert donc 1- la capacité d’enfiler un maillot, l’enzyme, et 2- le fait d’en avoir un sous la main, la vitamine C.
*On notera qu’une acidité gastrique adéquate est aussi impliquée dans l’altération de la charge du fer. Les individus sous administration d’inhibiteurs de pompe à proton (réducteurs d’acidité gastrique), devraient donc garder ce fait en tête quand ils évalueront leurs besoins1. La bactérie H.pylori peut aussi venir jouer sur l’absorption initiale du fer via un baisse d’acidité gastrique2.
Le fer Fe3+ ainsi converti en Fe2+ -équivalent de notre baigneur maintenant décemment vêtu- peut s’engager depuis l’intestin, dans la cellule intestinale via un transporteur (le DMT1).
Le fer étant dommageable pour l’organisme; il ne peut ressortir de l’autre côté de la cellule intestinale et gagner accès à la circulation que s’il est couplé à une molécule en quelque sorte « atténuante/ stabilisante/ désarmante » soit ::
Pour sa circulation HORS cellule :: il se lie à la transferrine, une protéine de transport, de transfert
Pour son stockage DANS une cellule :: il se lie à une ferritine, une protéine de réserve de fer
Il est à noter qu’encore une fois la charge du fer devra changer; le fer ne peut s’accrocher à aucune de ces molécules sous sa forme Fe2+. Notre baigneur en maillot est bien entré à la piscine, mais il doit maintenant revêtir un bonnet de bain pour gagner accès au bassin et finalement nager.
Deux molécules se chargent d’altérer, une fois de plus, la charge du fer; elles sont toutes 2 dépendantes du cuivre ::
Héphaestine :: travaille majoritairementà faciliter la sortie du fer des cellules intestinales où il a été absorbé initialement
Céruléoplasmine :: impliqué dans la facilitation de l’accrochage du fer à la transferrine se chargeant de son transport sécuritaire
Ces 2 composantes expliquent en partie que les gènes impliqués dans la gestion du cuivre soient régulés dans la même direction que ceux impliqués dans l’absorption du fer en cas de carence en fer3.
On récapitule ::
Le fer végétal, doit subir une réduction de charge pour pénétrer dans les cellules intestinales. Une enzyme, avec l’aide de la vitamine C, le converti. On s’imagine un baigneur nu à qui on demande de bien vouloir mettre un maillot pour entrer à la piscine publique.
Le fer maintenant dans la forme/ tenue appropriée, entre dans la cellule via un transporteur, une porte.
Pour gagner accès à la circulation et être ultimement utilisé ou stocké, le fer doit, une fois de plus, subir une altération de charge, une oxydation. Notre baigneur indécent repenti doit maintenant enfiler un casque de bain pour gagner accès à l’eau. Héphaestine et/ou céruléoplasmine, 2 protéines nécessitant du cuivre pour fonctionner, se chargent de cette altération.
Le fer maintenant dans la forme/ tenue appropriée est finalement utilisable par l’organisme.
On conclue que pour des raisons évidentes, les surcharges de fer végétal alimentaire (je ne parle PAS de suppléments!) sont très improbables. Le métabolisme est complexe et cela peut jouer, contrairement à la croyance populaire de « végé = carencé », en faveur de l’individu.
Abosorption du Fe2+/ Héminique
Le fer de source animale ayant déjà la bonne charge pour l’absorption intestinale -il arrive à la piscine DÉJÀ vêtu d’un maillot- emprunte simplement un transporteur, le HPC1. Notez qu’il emprunte une porte différente de notre ami nu, expliquant le fait que ces 2 formes de fer ne se font pas compétition pour l’absorption; chacun ont leur porte d’entrée spécifique.
Une enzyme, l’hème oxygénase, libère le fer de sa molécule de transport, l’hème. Analogie douteuse #2 :: notre baigneur arrivant en maillot porte aussi un manteau; il doit donc le laisser dans un casier dans le vestiaire. S’ensuit un mécanisme de circulation/ absorption, toujours dépendant du cuivre, identique à celui du fer végétal/ non héminique décrit plus haut.
Une fois l’étape initiale de l’absorption intestinale réussie (Maillot d’bain? Check. Manteau retiré? Check.), les 2 formes deviennent interchangeables via transfert d’électrons se faisant au gré des besoins en « stockage » et « utilisation » de l’organisme.
Régulation
Les cellules intestinales n’activent leurs transporteurs et récepteurs de fer que si elles ont reçu un message leur indiquant un besoin. Le nombre de transporteurs de fer n’est pas statique, il fluctue au gré de la régulation hormonale4,5.
C’est l’hepcidine, hormone hépatique maitresse de la régulation du métabolisme du fer, qui se charge de communiquer les besoins aux parties impliquées dans l’absorption et la circulation du minéral.
En cas de fer suffisant ou surprésent :: elle se fixe sur la ferroportine; le seul exportateur de fer connu situé à la surface des cellules. Elle provoque l’internalisation et la dégradation de ces portes de sortie du fer. En gros, elle baricade les ponts donnant accès à l’extérieur des lieux de stockage et « emprisonne » le fer dans les cellules. Elle limite ainsi une utilisation supplémentaire de fer qui pourrait s’avérer nocive.
En plus d’inhiber son relargage des lieux de réserve, l’hepcidine bloque également l’absorption intestinale du fer ; sa présence est donc logiquement élevée en cas de surcharge de fer.
Suivant cette ordre d’idée, un pool de fer insuffisant aura pour effet de diminuer la sécrétion d’hepcidine et permettra libération et absorption intestinale du fer sans restriction.
À noter :: Un état infectieux et/ou inflammatoire aura aussi un effet promoteur d’hepcidine. La régulation du fer n’est donc pas qu’une question de « fer suffisant ou pas», l’équilibre inflammatoire de l’organisme joue un rôle important dans la bonne gestion du fer via son effet sur l’hepcidine. Obésité, maladie auto-immune, pathologies entrainant des saignements chroniques ou une irritation constante de la muqueuse intestinale, grossesse, infection à Helicobacter pylori… ; plusieurs facteurs au-delà de la simple équation fer in/ fer out sont à prendre en compte quand on évalue les besoins en fer d’un individu.
Recyclage du Fer
Il n’existe aucun système actif d’excrétion du fer chez l’humain; le contenu en fer de l’organisme est principalement contrôlé par la modulation de l’absorption intestinale. Elle est tantôt accrue, tantôt ralentie, voire stoppée.
La régulation du fer est en quelque sorte quasi « auto-suffisante »; elle implique très peu d’entrée et de sortie du minéral puisqu’il est constamment recyclé/ réutilisé.
Des 3 à 5g présents dans un organisme sain, 99% ne peuvent en sortir; expliquant que les besoins quotidiens soient si minimes.
Sa répartition se décline ainsi ::
La production et maturation des globules rouges et leurs précurseurs dans la moelle osseuse accaparent les 2/3 du fer total de l’organisme; la majeure partie de ce fer provient du recyclage des globules rouges ayant atteint la fin de leur vie utile. Ce sont les macrophages du foie et de la rate qui sont en charge de la dégradation des globules rouges et du relargage du fer qu’elles contiennent dans la circulation.
Une partie du fer disponible est également stockée dans les cellules du foie par les ferritines.
Longévité
Contrairement à ce qu’on pourrait croire, la charge totale de fer dans l’organisme tend à augmenter au fil des ans6; les apports moyens de la diète Nord Américaine étant fréquemment plus importants que les besoins. Cette accumulation serait responsable d’un vieillissement cellulaire accéléré dû au stress oxydatifs engendré par la surprésence de fer dans l’organisme. Plusieurs études démontrent des dépôts de fer dans la substance noire d’individus affecté par la maladie de Parkinson7.
Une concentration en fer plus faible dans l’organisme pourrait en partie expliquer la longévité plus importante des femmes vs celle des hommes. Les saignements mensuels étant source de perte de fer; ils auraient possiblement un effet préventif sur l’accumulation de fer quasi inévitable chez l’homme. Les travaux du Dr Thomas Perls sur le sujet de la longévité sont particulièrement intéressant.
De plus en plus d’études soutiennent les sources végétariennes de fer comme “protectrices” de cet effet d’accumulation puisque malgré une abondance marquée dans l’alimentation, l’absorption est plus modeste, ce qui est bénéfique à un organisme sain et adéquatement alimenté et régulé8,9.
Alimentation AVANT supplémentation
On ne le répétera jamais assez, la supplémentation en fer n’est pas à prendre à la légère; un test sanguin reste la meilleure façon d’évaluer les besoins réels. Inquiets? Curieux? Une simple prescription d’analyse sanguine par votre médecin traitant reste l’avenue par excellence pour clarifier vos taux.
Cela dit, l’analyse de vos choix alimentaires et de votre état de vitalité générale sont aussi des outils inestimables dans la compréhension de vos besoins spécifiques.
Commencer par prendre connaissance des faits sur les apports sub-optimaux en fer en lisant cet article détaillant les différents mécanismes de l’anémie. Tout étant interrelié dans l’organisme humain; on se rend vite compte que le fer n’est pas un agent agissant seul dans le contexte de la santé sanguine. La vitamine C et le cuivre ont été mentionnés ici, mais la présence de plusieurs autres micronutriments (B6, B9 et B12 entre autres) est aussi cruciale dans la quête de bien-être absolu.
La « Fiche VBN – Fer » met en lumière les faits de bases couvrant pour les apports recommandés, les sources, les pertes possibles et les risques liés aux apports exagérés.
Quelques études sont intégrées à même cet article, n’hésitez pas à lire plus en profondeur sur le sujet; ce billet n’est qu’une synthèse rapide et simplifiée.
Si besoin il y a, envoyez ou présentez ces études à votre praticien de santé afin d’évaluer si vos taux de fer soutiennent pleinement votre vitalité.
Restons toujours humbles et curieux,
Soyez bien,
Vicky x
Vicky Bachand ND.A est naturopathe :: un naturopathe ne remplace pas un médecin.
Les renseignements contenus dans cet article sont présentés strictement à titre informatif et ne visent pas à fournir des renseignements complets sur les sujets traités ni à remplacer les conseils d’un professionnel de la santé qualifié.
Ces renseignements ne constituent ni une consultation, ni un diagnostic ou une opinion médicale, et par conséquent, ne doivent pas être interprétés comme tels.
Consulter toujours votre professionnel de la santé si vous avez des questions au sujet de votre état de santé.
No time to read!? Not thaaat interested in getting to know vitamin D “in depth”?! Then simply know and remember this one basic thing ::
Health Canada’s DRIs – Dietary Reference Intakes suggest daily intakes of 600IU of vitamin D for individuals aged 1 to 70. From that point, total goes up to 800IU for older adults. Any dose higher than these reference values should be evaluated by a health care professional.
There! These are the numbers that should cover the needs of the majority of healthy individuals who don’t have the opportunity to expose their skin to the sun sufficiently.
These suggested values represent a sufficient amount for most but not necessarily anoptimal one for all. Individualising these suggestions should be considered, but in order to do that, I’m afraid you’ll have to keep reading and/or meet up with a health specialist who can give you the blabla and save you the reading. 😉
There are 2 basic rules that define a “vitamin” ::
It is essential to reactions in the body
The body cannot produce it itself
Following this logic, one could argue vitamin D is either an exception or a labelling glitch; it’s actually most accurately described as a steroïd/ cholesterol based hormone.
Its production within the human organism, just like cholesterol’s, is absolutely possible; vitamin D is synthesized in the skin when it is exposed to UVB rays.
The sunshine vitamin comes in 2 forms ::
D2 :: ergocalciferol
D3 :: cholécalciferol
*If you are curious about all the pathways and structures involved in endogenous vitamin D production, read this piece :: ” Human body; a vitamin D production plant“.
Vitamin D’s main job is to regulate calcium and phosphate levels circulating in the body. Simply put, it has the power to boost these minerals’ absorption in the intestinal tract AND can release them from their storage organs, mainly, the skeleton.
It is estimated that vitamin D regulates more than 2 000 genes. Its receptors can be found in ALL tissues of the body, including the brain; thus, suggesting that its action goes far beyond mineral regulation. Adequate intakes of this vitamin seem to be linked to greater longevity1.
Main source
RESPONSIBLE exposition to the sun’s rays
While the sun’s rays have been demonized for a while now, I reckon it’s time to give them back the level of recognition they deserve.
Having full trust in the omniscience of Nature, I find it impossible to believe it would have elaborated such a complex and masterful mechanism of “in-house” production of vitamin D via the sun’s energy only to have us avoid sunbeams at all costs.
The sun is a FREE source of vitamin D and contrary to external supplementation, it plays harmoniously with our own self-regulating mechanisms.
*Bonus, sunlight has the power to replenish our CoQ10 stores; an antioxidant our cells use for growth and repair. It also acts favorably on blood pressure and arterial function by liberating a substance, nitric oxide, which is present in the blood stream after ingestion of nitrite/nitrate containing foods. Dark leafy greens and beetroot are great precursors of this phenomenon.
Emphasis should be placed on the fact the SUN’s rays are able to do all this, NOT isolated vitamin D supplementation2,3. Supplementation is not a bad idea, it simply should be done with a certain level of restraint and not be your only option and source of any nutrient.
Safely taking advantage of the sun’s rays
Therapeutic UV exposition should not be done between the hours of 10am and 4pm.
During these “high sun” hours, all public health recommendations should be followed :: hat, sunglasses, sun protection in the form of SPF30 minimum sunscreen and/or protective clothing4.
Photoaging, increased incidence of cataracts, damages to our DNA and skin cancers linked to IRRESPONSABLE sun exposure are not questioned here.
It is critical that we approach the sun’s beneficial and vitalizing rays in a judicious and parsimonious way.
A great (and dead simple!) indicator of UV rays’ strength is the following :: if your shadow is taller than your actual height, then sun protection might not be necessary. Once this ratio is equal or reversed and your shadow becomes shorter than you :: protection becomes mandatory5.
In Canada, on average, 10 to 25 minutes/ day of sun exposure without protection during the months representing spring and summer are sufficient to obtain adequat amounts of vitamin D.
Aspects influencing time of exposure ::
Skin colour :: darker skin typically requires more time
Age :: the older we get, the more time we need
Exposed surface area :: the more covered we are, logically the more time we need to allow sufficient production
In winter, considering roughly 10% of our bodies are exposed (face and possibly hands), required time in the sun goes up ::
At 10 :00 –> 9.7hrs would be necessary
At 16 :00 –> 5.7hrs would be necessary
The sun’s angle simply isn’t conducive to the production of significant amounts of the sunshine vitamin. These values being impossible to achieve, supplementation in localities north of latitude 37′, during the months representing winter, is very much suggested6,7,8.
Therapeutic exposition to the sun’s energy should not serve as a tanning tool. For those of us who enjoy a little tan ::
It is worth noting that regular consumption of carotenoids (dark leafy greens and orange hued fruits and veg) allows the body to create a similar pigmentation from within. Turns out it even is, apparently!?, even more attractive than its “sunbaking” counterpart.
Going full on “rotisserie chicken” mode in the sun for hours on end is guaranteed to bring about trouble in the long run. Smoothie drinking and enhanced physical fitness both actually offer increased vitality and a healthier glow which is just as attractive, if not more!, as skin damaging, overdone sun worshipping9,9A,9B.
Sources, D3 ::
Fish
Haddock :: chunks, 1 cup/ 136g – 32IU
Cod :: chunks, 1 cup/ 136g – 63IU
Eel :: chunks, 1 cup/ 136g – 572IU
Salmon :: chunks, 1 cup/ 136g – 473IU
Tuna (Albacore) :: chunks, 1 cup/ 136g – 109IU
Calve’s liver :: cooked, 136g – 234IU
Egg yolk :: 2 large, cooked – 72IU
D3 fortified products :: produced from lanolin (Extracted from sheep’s wool)
Microalgae that has been exposed to UV :: found in some vegan supplements
Lichen :: found in some vegan supplements
Sources, D2 ::
Certain mushrooms
Vitamin D concentration is conditional to UV exposure10 :: UV fungi are generally clearly identified on their label. Certain companies also offer UV treated, D2 rich, mushroom powder for culinary purposes. Mushrooms that are grown with standard “in-the-dark” processes are NOT a significant source of D2.
Portobello UV, raw :: 1 cup, diced/ 86g – 976IU
Cremini UV, raw :: 1 cup, diced/ 72g – 919IU
White button mushrooms, raw :: 1 cup, sliced/ 70g – 732IU
Fortified products or supplements enriched with a type of yeast (Saccharomyces cerevisiae) that has been exposed to UV light.
**While the D2 type, from food or supplements, has been shown to contribute to the elevation and maintenance of vitamin D levels in the body; the D3 form is thought to offer a slightly better efficacy when supplement forms are compared. Luckily, D3 supplements on the market today come from various sources. Omnis and vegans can find a suitable D3 product to suit their needs and ethics11.
Precautions
Certain foods that are rich in D are also highly concentrated in vitamin A. This vitamin, when ingested in excess, is associated with an increased risk of prostate cancer, cardiovascular disease and has shown deleterious effects in neurodegenerative conditions such as Alzheimer‘s and Parkinson‘s disease12.
A great example is cod liver oil :: each tablespoon will exceed both vitamin D and A recommended intakes. 1 tbsp represents 1 360IU of vitamin D (which is high but still below the maximal tolerated daily intake of 4 000IU) and 13 600IU of preformed vitamin A (Tolerable upper intake level :: 10 000IU!!). A daily consumption of such a food will quickly “pile on the excess” to your detriment.
An excessive intake of vitamin A is thought to disturb mitochondrial function and structure; mitochondria are the body’s tiny energy plants. Hair loss and/ or diarrhea are common signs of excessive intake of vitamin A.
People suffering from Williams Beuren syndrome or infantile idiopathic hypercalcemia both present anomalies in their regulation of calcium and vitamin D. They should definitely consult their doctors before supplementing either of these nutrients13.
Risks of exagerrated intakes
Vitamin D is a fat soluble substance; just like vitamins E and A, it is best absorbed and assimilated in the presence of fats and oils.
Unlike water soluble nutrients which can be excreted in urine when the body has more than it knows what to do with; excess vitamin D intakes end up being stored in the fatty tissue of our bodies where it accumulates.
Exaggerated intake of vitamin D supplements, and the saturation of our fat cells, can result in a blood level exceeding the upper limit of 150nmol/L. This (avoidable) imbalance can lead to an overabundance of calcium in the body, calcification of tissues and calcium deposits in tissues where it does not belong and dehydration.
Dietary intake and responsible sun exposure are the best ways to fulfill the body’s needs while avoiding deleterious effects.
Superfluous vitamin D in the body can translate into the following signs :: confusion, apathy/ lethargy, vomiting, abdominal pain, frequent urination and thirst that is intense and difficult to quench (polyuria/ polydipsia). Note :: redundant over supplementation of vitamin D during long periods of time could increase certain cancer risks (pancreas, breast, prostate) and all-cause mortality 14,15.
Sub-optimal intakes and associated risks
Demineralisation of bones and increased risk of fracture
While establishing a distinction between sun exposure and adequate vitamin D levels might not always be obvious or even feasible, links between inadequate vitamin D levels and certain conditions and discomforts have been suggested and are presently being studied16 ::
In growing children and adolescents, rickets is to be kept in mind :: the condition is linked to poor bone quality characterised by osteomalacia (soft bones) and osteoporosis (fragile bones). It is tightly linked to a mineralisation deficit of the skeleton.
Specific needs
Menopausal women
Young children :: breastfeeding women should shave their vitamin D tested, support its adequate concentration and should consider a source of supplementation for their infant/ child.
Obese individuals :: vitamin D having such a strong affinity for adipose tissue, it could end up being sequestered in fat cells before it can meet the receptors that are responsible for its activation.
Inversely, an obese individual on a weight loss journey could see their vitamin D level naturally rise as fat (and the stored vitamin D within it!) is released from storage. Supplementation in this case would be futile.
Elderly population :: diminished renal function, decreased presence of precursors within the skin, limited sun exposure and reduced appetite can all impact vitamin D intake and assimilation.
Dark skinned individuals :: the important presence of pigments in the skin makes photoproduction of vitamin D a touch more difficult.
Individuals with conditions that make the digestion of fat difficult such as those diagnosed with Crohn‘s or celiac disease. Vitamin D’s absorption being linked to presence of fat in the diet, optimal absorption might be compromised.
Persons taking glucocorticoid type medication (prednisolone/ prednisone, hydrocortisone…) should consult their doctors and evaluate their needs to avoid glucocorticoid induced osteoporosis.
People suffering from known malabsorption issues should also consult with their medical doctors to evaluate their needs.
While evaluating vitamin D needs, the following elements should be kept in mind ::
Country of residence’s latitude. Montréal is located at latitude 45’, and therefore follows general sun exposure guidelines referring to latitudes comprised between 40’ and 50’.
Time of year :: from April to October, the sun’s angle is favorable to adequate cutaneous production of vitamin D. From November to March however, people residing north of the 37e parallel should consider supplementing their diet19.
Lifestyle and time spent outdoors during months when endogenous production is possible.
Skin color :: the lighter the skin, the easier the internal production, the smaller the needs.
Age :: as skin atrophies with time’s passing, vitamin D production becomes less and less efficient. Absorption through diet also decreases with age20.
Actual consumption of “natural” and fortified vitamin D sources.
Vitality of organs involved in vitamin D activation :: liver and kidneys. A diagnosed pathology of either of these structures requires medical advice. Naturopathy can most definitely tag along as a vitality support and prevention of function decline modality.
Integrity of parathyroid glands regulating PTH hormone. A diagnosed pathology of these structures requires medical advice. Naturopathy can most definitely tag along as a vitality support and prevention of function decline modality.
Bone density and all lifestyle and dietary factors that could influence it.
Other supplements being taken regularly. Ex. :: isolated calcium supplementation could lead to kidney stones.
One has to remain smart, educated and somewhat timid when considering supplementation :: it is NOT a panacea. Numerous studies have attempted to link “vitamin D supplementation and healing properties” and could not put forth a strong correlation.
Vitamin D is first and foremost and prevention tool and “more” most definitely is not automatically linked with “better”.
Blood tests
*Blood tests are prescribed and interpreted by medical doctors. Total vitamin D can be included in blood tests, all you have to do is ask.
Reference values ::
75 to 150nmol/L is considered ideal.
50 to 74nmol/L reads as “insufficient”
50nmol/L or less, reads as a “deficiency”
As with most things related to health, this one blood value is not enough to evaluate needs and actual state of vitality; other aspects must be investigated to round out the results.
*I think it is also worth mentionning that African tribes living an “ancestral lifestyle” have been studied in the context of vitamin D levels :: Massaii and Hadzabe tribes live a life that is very active, quasi nude and abundantly exposed to the sun year round at a latitude that is conducive to uninterrupted vitamin D production in the skin. This demographic presents average vitamin D levels around 115nmol/L. One could hypothesize this value to be what nature had in mind when it created human beings as self-regulating vitamin D production entities; we should therefore keep the door open to further studies that could define optimal levels closer to this figure in the futur22.
A few precisions on dosage, timing of ingestion and supplement choice
According to a study from the Journal of Bone and Mineral Research, most studied individuals achieve adequate vitamin D levels with a daily intake of 400 to 600IU for children and around 800IU for adults.
Data suggests that doses as high as 1000IU for children and 2000IU for adults (obviously depends on individual profiles) are well tolerated and safe for long term use in most cases23.
Taking a vitamin D supplement WITH the largest meal of the day seems to boost absorption24.
Dietary supplements are most definitely not all created equal. One should look for a lab that opts for third party testing to confirm the accurate concentration and quality of its product.
There we have it :: vitamin D in a nutshell!
A few studies have been linked throughout this article, get acquainted with the data if you wish to know more about this topic; this post is merely a quick and simplified intro into the subject.
Research papers are always a great way to approach a discussion with your health care provider, feel free to share them with yours if you think it would be useful in the evaluation of your specific needs and the enhancement of your vitality.
Stay curious and humble,
Be well,
Vicky x
Vicky Bachand ND.A is a naturopath :: a naturopath does NOT replace a medical doctor.
Ideas provided in this article are presented as information only and do not aim to provide in depth details about the chosen topic nor replace the advice of a qualified health care provider.
Information shared here does not constitute a consultation, a diagnosis nor a medical opinion and therefore should not be interpreted as such.
Always consult with your chosen health care provider if you have questions about your personal health.
Should you read or remember only ONE thing from this piece, it should be the following ::
Iron is both ESSENTIAL and TOXIC to the human body.
In a society where most people seem to think “if a little is good, than moore must be better” I truly wish to place emphasis on the fact that this motto cannot be applied to most of our metabolic needs and processes.
The human body was created to constantly and tirelessly dissipate the excesses and insufficiencies that our chosen lifestyles generate. Why in the name of Life anyone would aim to overburden such a beautiful machine is beyond me?!
Isolated iron supplementation should be done using a “Goldielocks” approach; it is not recommended to all and the guidance of a health care professional is very much advised.
Notoriously hard to absorb, iron is also pretty hard to get rid of. A poorly informed, “self-supplementation regimen” could place a well-meaning individual in a deleterious state of overconsumption and absorption.
Iron has many uses within the body ::
Oxygen transport
Electron transfers
Cellular respiration –> energy production!
Synthesis and repair of DNA and various proteins
RNA synthesis
It is a cofactor of numerous enzymes :: enzymes which are essential to ALL human biochemical reactions
Necessary to the production of hemoproteins :: hemoglobin, myoglobin, cytochromes…
When in excess and/or in a case of compromised regulation, it can disrupt wellbeing ::
It promotes the formation of ROS, Reactive Oxygen Species. These molecules can cause damage to DNA and/or inactivate certain enzymes. In simple terms, think :: toxic free radicals. Poorly regulated and/or excessive circulating iron levels can cause premature, accelerated cell aging. (Fenton’s reagant)
This important mise-en-garde out of the way, we can now discuss how the human body regulates its iron supplies.
Intakes
Iron is a mineral that is deemed “essential” :: the body cannot produce it therefore, dietary sources must be consumed.
There are 2 forms of iron available in food ::
**An important distinction vegetarians and vegans will want to pay attention to :: absorption pathways of these 2 minerals are different, and the quantities absorbed are not the same either.
Ferrous Iron/ Fe2+/ heme iron :: Makes up 10% of dietary iron and represents 1/3 of all absorbed iron. This form comes from animal sources which package the mineral in hemoglobin and myoglobin that is similar to ours. “Heme iron” confirms that the iron is located within a heme protein. We could compare this type of iron to a guy (iron) arriving at the public pool (human bloodstream) wearing a jacket (heme) on top of his bathing suit. Stick with me, I hope this makes things clearer for us later! 😉
Ferric iron/ Fe3+/ Non heme iron :: Makes up about 90% of dietary iron and represents 2/3 of all absorbed iron. This inorganic form mainly comes from plant sources. It is not packaged in heme it is more like a swimmer arriving at the public pool buck naked! No coat, no bathing suit! I’m sure you see why SOME alterations will have to happen to this guy before he can gain access to our blood pool.
Absorption of NON heme Fe3+ iron :: the one that requires vitamin C
In the intestinal tract, ferric iron from plant sources cannot “simply” be absorbed; an enzyme must first alter its charge, that little number floating at the top right of the Fe (enzyme DCYTB, mainly). This enzyme requires vitamin C to operate. If you’ve ever heard that it’s beneficial to combine plant iron sources with vitamin C rich foods :: this is why!
NO vitamin C means NO charge alteration which in turn means NO absorption
If we go back to our dodgy analogy, this “charge alteration” is a bit like asking naked guy to put on a suit before entering the premises. Entrance is therefore conditional to 2 criteria :: 1 – having the ability to get dressed, the enzyme and 2- having a bathing suit on hand, vitamin C.
*It is worth mentioning that adequate stomach acid (low pH) also plays a role in the alteration charge of iron. People on proton pump inhibiting medication, which reduce gastric acid (up the pH), should keep this is mind when evaluating their needs1. H. pylori bacteria is also known to throw off our ability to absorb iron through its pH rising effect on stomach secretions2.
Fe3+ iron now converted into Fe2+ -our naked bather in appropriate public pool attire- can travel form the intestines into intestinal cells via transporters/ doors (DMT1).
Iron being highly reactive and actually damaging to the human body in its free form; it can only be allowed to travel from the intestinal cell into circulation once coupled with a “stabilising/ disarming/ mitigating” molecule ::
For its circulation out of the intestinal cell into the bloodstream :: transferrin is in charge, it is a transport or transfer protein.
For its storage inside our cells :: it gets bound to ferritin, an iron reserve protein
Once again, iron’s charge will have to be altered. Iron cannot bind to neither transferrin or ferritin in its newly acquired Fe2+ form. Our naked swimmer might be wearing a suit now, but he will not gain access to the water unless he’s wearing the mandatory bathing cap.
Iron assimilation :: a copper dependant step
Hephaestin :: who’s main job is to facilitate the iron’s exit from the intestinal cell where it was absorbed initially
Ceruloplasmin :: which is in charge of facilitating iron’s binding to transferrin for its safe blood transport
These 2 components partly explain why genes that are implicated in copper regulation react similarly to those regulating iron in a deficiency situation3.
Recap ::
Iron from plant sources must have its charge altered in order to gain access to intestinal cells. An enzyme, with vitamin C’s help, is in charge of converting Fe3+ iron into Fe2+iron. We can imagine a naked person wanting to gain access to a public pool, the charge altering can be imagined as a change into proper, non-naked attire.
Iron, now in its “bathing suit form”, enters the cell via a transporter.
To gain access to the bloodstream and ultimately be used or stored iron must, for the second time, have its charge altered. Our swimming enthusiast must now put on his bathing cap before he can dip his toe in the water. Hephaestin and ceruloplasmin, 2 proteins that rely on copper, are in charge of this step.
Iron is now perfectly configured to be used by the body however it pleases.
It is logical to conclude that overconsumption of iron via dietary PLANT sources is highly improbable (NOT talking about supplements here!). This complex mechanism has a protective effect on our constitution :: plant iron being a common occurrence, its complete and full absorption at all times could have harmful effects.
Absorption of heme/ Fe2+ iron :: no vitamin C required!
Iron form animal sources comes already with the charge required for intestinal absorption :: he’s just that decent guy who arrives at the pool ALREADY wearing a bathing suit. This type of iron simply uses a transporter to get into our cells (HPC1). Both types of iron have their own specific transporters and that is a good thing because it means there is no competition for the entryway. A public pool has more than one door, and each bather has its fave. There, no fighting!
Once Fe2+iron is inside the intestinal cell, an enzyme, heme oxygenase, proceeds to free it from its heme packaging. Still going with our pool/ bathers’ analogy, then “enzyme & heme” combo would best be represented by a jacket (heme) that one would leave in a locker (enzyme). Our iron, guy coat free and in his swimming trunks is ready to go and will then follow the same steps as the other form of iron previously described :: bathing cap/ copper dependence, proteins to keep it safe within the bloodstream…
As we can see, both forms become interchangeable once the initial absorption is over. Bathing suit? Check. Coat left in the locker? Check. From that point on everyone can act the same :: put your bathing cap on and proceed. Charges are altered following the body’s cues, both iron forms able to go from the “stored” form to the “use up” form with the help of enzymes and copper dependant carrier proteins.
Regulation
Intestinal cells will only “activate” their iron receptors if they have received a signal to do so. The number of receptors on the cells’ surface is not static but fluctuating in accordance with hormonal messaging4,5.
It is hepcidin, liver hormone master of iron regulation, who’s in charge of communicating metabolic needs to all the parts involved in iron absorption and circulation.
When iron is sufficient or overabundant :: hepcidin binds to ferroportin; the one known iron exporter which is located on the cells’ surface. Hepcidin causes internalisation and degradation of said iron exit doors. It sequesters iron INSIDE the cells by burning all the bridges giving it access to our circulatory system and tissues in order to limit its use and accumulation and prevent an adverse outcome.
Not only does it imprison iron inside storage cells, hepcidin also blocks intestinal absorption; hepcidin secretion is increased when iron is sufficient or overabundant.
Inversely, an inadequate iron pool will cause a decrease in hepcidin secretion, allowing unrestricted intestinal uptake and improved liberation of stored iron for usage.
Worth mentioning :: An infectious and/or pro-inflammatory state has a promoting effect on hepcidin. Iron regulation is therefore not ONLY an “iron in/ iron out” mechanism. Acute or chronic inflammation plays an important role on proper iron regulation via its effect on hepcidin. Obesity, auto-immune conditions, pathologies involving chronic blood loss and/or constant irritation of the intestinal mucosa, pregnancy, H. pylori infection… All of these conditions have some type of direct or indirect effect on an individual’s iron stores.
Iron recycling
There is NO known active iron excretion mechanism in humans. Iron that is present in the body is primarily regulated via intestinal absorption modulation; it is increased at times and slowed or stopped during others.
This regulation can be described as “self-sufficient”; it requires very little iron entry or excretion since it is constantly being reused/ recycled.
Of the 3 to 5g of iron present in a healthy body, 99% will never find the exit; explaining why we have such minimal daily dietary requirements.
Within the body, iron is distributed in these ways ::
Production and maturation of red blood cells and their precursors in the bone marrow “hog” 2/3 of all iron stores; the majority of which comes from the recycling of red blood cells that had reached the end of their useful lifespan. Macrophages from the spleen and liver are in charge of red blood cell degradation and recirculation of their useful components.
A fraction of available iron is stored as “ferritin” within liver cells.
Longevity
Contrary to what one might think, the total concentration of iron within the body tends to increase with the years6; the average North American diet frequently providing more than is necessary. This accumulation is thought to be partly responsible for premature or accelerated cell aging due to the oxidative stress it generates. A few studies have shown iron deposits within the brain’s dark matter (substantia nigra) of individuals suffering from Parkinson‘s disease7.
A lesser concentration of iron such as the one usually found in women who menstruate, could partially explain why feminine longevity is greater than men’s. Periodic, monthly bleeding representing regular iron losses; it could possibly have a preventative effect on excessive iron concentrations. Dr Thomas Perls‘ research work on this topic (and longevity in general) is particularly interesting.
More and more studies seem to define vegetarian sources of iron as “protective” from this accumulation phenomenon; despite an abundance of iron in the veg diet, the absorption rate remains modest. What we assumed just a few years ago to be a “miss” for vegetarians is slowly turning out to be an advantageous, built-in regulation system that brings benefits in the long run for those consuming an adequate, properly planned, plant rich diet8,9.
Dietary sources BEFORE supplementation
I’ll say it one more time :: isolated iron supplementation is not a thing to be done haphazardly; a blood test is one of the great tools when evaluating your needs. Worried? Curious? A simple blood draw prescription from your MD is an excellent way to begin your investigation.
That being said, the values from a blood analysis are only one piece of the puzzle :: your dietary choices, your general state of vitality and other lifestyle particularities are invaluable tools in the comprehension of your specific needs.
If you wish to know more about the implications of chronic sub-optimal iron intakes, maybe you’ll enjoy reading this piece on anemia.
All bits influencing all parts at all times within our bodies, it is foundational to understand that iron does not work alone. vitamin C and copper were mentioned here but B6, B9 and B12, among others, are also of capital importance on the journey towards proper iron metabolism, abundant energy and deep-rooted wellbeing.
The « VBN Sheet – Iron » sheds light on all basic facts about this important mineral :: daily reference intakes, sources, possible losses and risks linked to overdoing it are all discussed there.
A few studies have been linked through this article, get acquainted with the data if you wish to know more about this topic; this post is merely a quick introduction, a simplified intro into the subject.
Research papers are always a great way to approach a discussion with your health care provider, feel free to share them with yours if you feel it would be useful in the evaluation of your specific needs and the enhancement of your vitality.
Stay curious and humble,
Be well,
Vicky x
Vicky Bachand ND.A is a naturopath :: a naturopath does NOT replace a medical doctor.
Ideas provided in this article are presented as information only and do not aim to provide in depth details about the chosen topic nor replace the advice of a qualified health care provider.
Information shared here does not constitute a consultation, a diagnosis nor a medical opinion and therefore should not be interpreted as such.
Always consult with your chosen health care provider if you have questions about your personal health.
You reading this tells me you’re interested in preventing anemia; you might already know about the importance of certain nutrients such as B6, folate (B9), B12 and iron. If it’s not the case, you might find reading my piece “Anemia 101” interesting.
So, “sunshine vitamin” and iron metabolism :: what’s the deal?
Recent studies suggest ::
Vitamin D plays a role in diminishing molecules that work to promote inflammation (cytokines, small proteins involved signaling where/ when an inflammatory reaction is needed)
It acts as a suppressing agent of hepcidin; hepcidin being the CHIEF hormone of iron metabolism regulation
These 2 factors act in a favorable way on iron bioavailability in the human organism1 and support its equilibrium.
Hepcidin
Hepcidin, rarely discussed when “iron stores and utilisation management” is addressed in mainstream media, can be summed up like this ::
A hormone that is produced in the liver and secreted into blood circulation.
It acts as a NEGATIVE regulator of iron absorption and recycling.
i.e. :: it controls transporters (ferroportin) that allow iron to travel from cells –> to plasma.
It’s role :: inhibit iron absorption when its concentration in the body is optimal in order to avoid excesses that would throw the body off balance
Inflammation, infections and accumulation of iron in tissues increase hepcidin production.
During an infection, this protection mechanism triggered by pro-inflammatory molecules works to deprive invading organisms of iron in order to prevent their growth.
However, in a chronic inflammatory state*, this process that aims to reduce available/ circulation iron can bring about “shortages” in the production of hemoglobin and red blood cells which can lead to anemia.
NO iron :: NO hemoglobin. Iron is an important component of the hemoglobin molecule.
Inadequate production of hemoglobin translates to insufficient oxygen transport to the organs that need it.
*Obesity is considered a chronic inflammatory stateA.
Iron depletion can range from asymptomatic to debilitating. Find a list of symptoms here.
Vitamin D plays a supporting role in the production of red blood cells and hemoglobin
In a normal situation :: after a meal, as required by the body, a certain proportion of ingested iron is absorbed in the duodenum.
In an individual with a smooth operating constitution, iron is stored in the liver, to be used when needed and ultimately, recycled.
When red blood cells have reached the end of their programmed “life”, which is about 120days, they’re broken down into their various components (mainly globin, heme and iron). Iron is either stored or returned to circulation where it can reach bone marrow and be used in red blood cell production once again.
An inflammatory state (characterised by IL-6 et IL-1β) triggers the liver into producing more and more hepcidin. Hepcidin rising concentrations prevents iron stored in cells from “leaving” by binding (and ultimately breaking down) the bridges through which iron can flow into the plasma (ferroportin).
The anti-inflammatory power of vitamin D may help protect the individual from iron depletion in the following ways ::
A reduction in pro-inflammatory molecules which reduces hepcidin secretion. Reminder :: high levels of hepcidin makes utilisation of iron difficult or impossible.
A reduced hepcidin secretion restores iron bioavailability and promotes the production of red blood cells and hemoglobin via restoration of the iron recycling cycle.
An increased red blood cell production in turn, helps reduce hepcidin secretion, reinforcing the action just described.
Optimal intake of vitamin D acts favorably on iron metabolism in the following ways ::
Suppresses ARNm transcription of hepcidin.
Promotes ARNm expression of ferroportin.
Decreased levels of hepcidin and increased presence of ferroportin translates to the improvement of iron recirculation in the body; it increases its availability for hemoglobin and red blood cell production.
In a study published in the Journal of the American Society of Nephrology, healthy volunteers who were administered 100 000IU of a synthetic form of D2 saw their serum levels of hepcidin plummet in 24hrs. Similar results were observed on chronic renal disease patients undergoing dialysis2.
Adequate levels of Vitamin D assists red blood cell production (erythropoïesis) in 2 ways ::
It triggers BUF-E, Burst-Forming Unit-Erythroïd – proliferation. BUF-E are, in layman’s terms, red blood cell precursors. *Bonus :: BUF-E produce regulators that help to lower hepcidin!
Vitamin D is a promoter of the hormone responsible for activating red blood cell formation (Erythropoietin)3.
Literature on vitamin D defines its effects a little more each year ::
Yes! Vitamin D is great for bone health… And so much more!
Vitamin D holds important anti-inflammatory properties and supports, directly and indirectly, iron regulation which is of capital importance in red blood cell and hemoglobin production.
In a nutshell , vitamin D in the context of anemia prevention does the following ::
Decreases ::
Decreases pro-inflammatory molecules that trigger hepcidin secretion
Decreases hepcidin, which is an inhibitor or iron utilisation
Decreases erythropoietin resistance; the hormone that stimulates red blood cell production
Increases ::
Increases serum iron which, available through circulation, can be used and recycled
Increases production of hemoglobin; an oxygen (and CO2) transporter
Increases proliferation of erythroid progenitors (BUF-E), red blood cell precursors
Increases concentration of red blood cells
Increases erythropoietin secretion
Various studies corroborate these hypotheses :: insufficient intakes of vitamin D in children under the age of 24months4, in the elderly population5, in people suffering from chronic renal disease6 or suffering from cardiac insufficiency7 were all linked to an increased incidence/ risk of anemia. This association is even stronger in the case of inflammatory pathologies such as irritable bowel syndrome, ulcerative colitis, rheumatoid arthritis, Crohn‘s disease et systemic lupus erythematosus8.
Keeping in mind vitamin D synthesized in the skin is only a precursor and requires a 2 step activation process :: first through the liver, second through the kidneys; the vitality of these 2 organs should be taken into account when evaluating your needs.
Healthy individuals should simply aim for adequate intakes; massive doses do not benefit iron metabolism any more than simple “needs are met” quantities.
If you have no clue what your vitamin D recommended intakes are, you can get the info right here. My “VBN – Vitamin D Form” gives details about requirements, sources, depletion interactions and possible risks associated with unnecessary high dosages.
A few studies have been linked through this article, get acquainted with the data if you wish to know more about this topic; this post is merely a quick introduction, a simplified intro into the subject.
Research papers are always a great way to approach a discussion with your health care provider, feel free to share them with yours if you feel it would be useful in the evaluation of your specific needs and the enhancement of your vitality.
Stay curious and humble,
Be well,
Vicky x
** Not discussed here but relevant to circulating vitamin D levels and thus, to the prevention and management of anemia ::
FGF-23 – Inhibitor of kidney conversion of vitamin D. Produced by the kidneys and generally elevated in people suffering from chronic kidney disease.
PTH – Promoter of vitamin D conversion in the kidneys. Produced and regulated in healthy parathyroid glands.
Vicky Bachand ND.A is a naturopath :: a naturopath does NOT replace a medical doctor.
Ideas provided in this article are presented as information only and do not aim to provide in depth details about the chosen topic nor replace the advice of a qualified health care provider.
Information shared here does not constitute a consultation, a diagnosis nor a medical opinion and therefore should not be interpreted as such.
Always consult with your chosen health care provider if you have questions about your personal health.
Vous souffrez, ou avez souffert d’anémie et les solutions offertes par votre praticien de santé se sont limitées/ se limitent à la supplémentation en fer isolé
Vous êtes enceinte ou venez de donner naissance et souhaitez vous prémunir contre un état anémique possible
Vous êtes affligé d’une maladie inflammatoire et/ou auto-immune ayant la particularité d’engendrer des carences en fer
Végétarien ou végane, vous êtes soucieux d’un risque accru de carence en fer
Si vous vous reconnaissez dans l’un de ces scénario, ce qui suit est pour vous.
Si la prévention de l’anémie vous préoccupe, vous comprenez peut-être déjà l’importance des apports en B6, folate (B9), B12 et fer. Si ce n’est pas le cas, lisez ici mon papier intitulé « Anémie 101 ».
Alors, la “vitamine soleil” en lien avec le métabolisme du fer, en avez-vous entendu parler?
Des papiers récents suggèrent ::
Qu’elle jouerait un rôle dans la réduction de molécules engendrant l’inflammation (les cytokines, de petites protéines de signalisation)
Et agirait comme agent inhibiteur de l’hepcidine, une hormone provenant du foie, régulatrice MAITRESSE de la gestion du fer dans le corps humain
Ces 2 facteurs agiraient favorablement sur la biodisponibilité du fer dans l’organisme1et soutiendraient le bon équilibre de ce minéral.
L’Hepcidine
L’hepcidine, trop peu discutée dans la gestion du fer « grand public », se résume sommairement comme suit ::
C’est une hormone produite au foie puis sécrétée dans la voie sanguine.
Elle est responsable de la diminution de l’absorption et du recyclage du fer.
C.-à-d. :: elle contrôle les transporteurs (ferroportine) qui font passer le fer de ces lieux de stockage et d’asborption –> vers le plasma sanguin. Sans elle, le fer est et reste “séquestré” là où il est emmagasiné.
Son rôleprincipal :: prévenir l’absorption de fer excédentaire lorsque sa concentration dans l’organisme est suffisante. Elle veille à éviter les surcharges.
L’inflammation, les infections et une accumulation de fer dans les tissus font augmenter la sécrétion d’hepcidine.
En situation d’infection, ce mécanisme de protection a pour but de priver de fer des organismes envahisseurs afin de prévenir leur croissance.
En état d’inflammation chronique* par contre, ce phénomène de diminution du fer circulant devient persistant. L’état chronique, maintenu par l’abondance de molécules pro-inflammatoires, peut engendrer des déficits de production d’hémoglobine, de globules rouges et ultimement, entrainer l’état anémique.
PAS de fer :: PAS d’hémoglobine puisque le fer est un atome essentiel à la protéine d’hémoglobine.
Une production d’hémoglobine appauvrie signifie un transport d’oxygène inadéquat vers les organes qui en ont besoin.
*L’obésité est considéré comme un état inflammatoire chroniqueA.
L’état varie d’asymptomatique à grave, liste des symptômes ici.
La vitamine D jouerait un rôle de soutien dans la production de globules rouges et d’hémoglobine.
En situation normale :: suite à un repas, une certaine proportion du fer ingéré est absorbé dans l’intestin au gré des besoins de l’organisme.
Dans un organisme sain, simplement, le fer est soit stocké au foie, soit utilisé puis, ultimement, recyclé.
Quand les globules rouges atteignent la fin de leur vie utile, il sont dégradés en leurs différentes composantes (globine, hème et fer) et le fer est à nouveau, soit stocké, soit réacheminé dans la circulation où il peut rejoindre la moelle osseuse et être réutilisé dans la fabrication des globules rouges.
Hors, un état inflammatoire (impliquant IL-6 et IL-1β) stimule le foie à produire une plus grande quantité d’hepcidine. Cette forte concentration empêche la sortie du fer stocké en se collant puis en dégradant les transporteurs dédiés à la sortie du fer vers le plasma (ferroportine).
Un apport adéquat en vitamine D, aux propriétés anti-inflammatoires bien documentées, a démontré un effet stimulant la production de globule rouge via la diminution de molécules engendrant l’inflammation.
L’effet anti-inflammatoire de la vitamine D contribuerait de ces façons à prémunir l’individu contre l’anémie ::
Une diminution des molécules pro-inflammatoires ferait diminuer la sécrétion d’hepcidine qui, lorsqu’élevée, rend l’utilisation du fer difficile, voire impossible.
La sécretion d’hepcidine diminuée rétablirait la disponibilité du fer dans l’organisme et stimulerait la production de globules rouges et d’hémoglobine via la restauration du cycle d’utilisation et recyclage du fer.
Une production de globule rouge accrue engendrerait à son tour une diminution de la sécrétion d’hepcidine; renforçant l’action tout juste décrite.
Un apport optimal en vitamine Daurait les effets suivants sur la gestion endogène du fer ::
Suppresseurs de transcription d’ARNm dictant la production d’hepcidine qui elle, tend à rendre le fer inaccessible
Promoteurs d’expression d’ARNm exprimant la ferroportine qui elle, est favorable à la bonne circulation du feret favorise son utilisation par l’organisme.
Selon une étude tirée du Journal of the American Society of Nephrology, des volontaires sains auxquels on a administré 100 000IU de D2 de synthèse ont vu leur taux sérique d’hepcidine diminué en 24hrs. Des résultats similaires ont été obtenus chez des patients sous dialyse, atteints de maladies rénales chroniques2.
La vitamine D serait également un élément de support dans la production de globule rouge (érythropoïèse) de 2 façons ::
Elle accroit la prolifération de BUF-E, Burst-Forming Unit-Erythroïd – qui sont en termes simples :: précurseurs de globules rouges. *Bonus :: Ces précurseurs produisent des régulateurs qui ont pour fonction de réprimer la sécrétion d’hepcidine!
Elle présente un effet promoteur de l’hormone stimulant la production de globules rouges (érythropoïétine); facteur de croissance indispensable à la prolifération des précurseurs de cellules sanguines stimulant la production de globule rouge dans la moelle osseuse mentionnées ci-haut3.
La littérature est donc de plus en plus claire ::
Oui, la vitamine D pour la santé osseuse! Mais :: bien plus que ça!
La vitamine D détient une action anti-inflammatoire importante et soutient définitivement la bonne gestion du fer, des globules rouges et de l’hémoglobine dans le corps humain et ce, de façon directe et indirecte.
En somme, la vitamine D, dans le contexte de prévention et gestion de l’anémie ::
Diminue ::
Diminue les molécules pro-inflammatoires qui font augmenter la production d’hepcidine
Diminue la production et sécrétion de l’hepcidine qui elle, est un obstacle à l’utilisation du fer
Diminue la résistance à l’hormone stimulant la production de globules rouges dans la moelle osseuse, l’érythropoïétine
Augmente ::
Augmente le fer circulant qui lui, peut être adéquatement recyclé et/ou intégré aux tissus appropriés
Augmente la production d’hémoglobine, transporteur d’oxygène (et de CO2)
Augmente la prolifération de progéniteurs érythroïdes (BUF-E) –> précurseurs de globules rouges
Augmente la présence de globules rouges
Augmente la production de l’hormone stimulant la production de globules rouges, l’érythropoïétine
Des études variées corroborent ces hypothèses :: des apports insuffisants en vitamine D chez les enfants de moins de 24mois4, les personnes agées5, les personnes atteintes de maladies rénales chronqiues6 ou souffrant d’insuffisance cardiaque7 sont liés à un risque accru d’anémie. L’association est plus forte encore, en pathologies inflammatoires tels syndrome du colon irritable, colite ulcéreuse, arthrite rhumatoïde, maladie de Crohn et lupus érythémateux systémique8.
Compte tenu que la vitamine D produite par la peau est inactive et qu’elle doit être activée en 2 étapes :: au foie puis aux reins, la vitalité de ces 2 organes est à prendre en considération lorsque vous évaluer vos besoins.
Les individus sains devraient veiller à ce que leurs apports soient simplement suffisants; des apports excédentaires n’ont pas d’effet « extra » sur le métabolisme du fer.
Dans le néant quant à vos besoins en vitamine D :: lisez la « Fiche VBN – Vitamine D » pour connaître apports, sources, pertes possibles et risques d’apports exagérés.
Quelques études sont intégrées à même cet article, n’hésitez pas à lire plus en profondeur sur le sujet; ce billet n’est qu’une synthèse rapide et simplifiée.
Si besoin il y a, envoyez ou présentez ces études à votre praticien de santé afin d’évaluer si vos apports en vitamine D soutiennent pleinement votre vitalité.
Restez humbles et curieux,
Soyez bien,
Vicky x
** Non discutés ici mais influant les taux circulant de vitamine D et qui par défaut, peuvent avoir un rôle à jouer dans la prévention et gestion de l’anémie ::
FGF-23 – inhibiteur de conversion de la vitamine D aux reins, synthétisé aux reins et en général élevé chez les personnes atteintes de maladies rénales chroniques.
PTH – stimulante de synthèse de vitamine D aux reins, produite et régulée par les parathyroïdes saines.
Vicky Bachand ND.A est naturopathe :: un naturopathe ne remplace PAS un médecin.
Les renseignements contenus dans cet article sont présentés strictement à titre informatif et ne visent pas à fournir des renseignements complets sur les sujets traités ni à remplacer les conseils d’un professionnel de la santé qualifié.
Ces renseignements ne constituent ni une consultation, ni un diagnostic ou une opinion médicale, et par conséquent, ne doivent pas être interprétés comme tels.
Consulter toujours votre professionnel de la santé si vous avez des questions au sujet de votre état de santé.