Plusieurs faits à savoir, mais pas tous!, sur les apports en fer sont listés sur cette page :: les apports recommandés, les causes de “pertes”, les effets d’apports insuffisants, les dangers de la SURsupplémentation et/ou d’apports exagérés et quelques trucs pour maximiser l’absorption.
Les ANREF – Apport Nutritionnel de Référence de Santé Canada suggèrent les apports quotidiens suivants::
- Hommes, adultes et enfants :: 8mg/ jour EXCEPTION faite des adolescents de 14 à 18 ans pour qui les besoins s’élèvent à 11mg/ jour.
- Femmes, les besoins dépendent de l’âge :: de 9 à 13 ans et pour les femmes de plus de 51 ans; les besoins sont de 8mg/ jour.
- Adolescentes (14-18):: 15mg/ jour
- Femmes adultes qui ont des règles (19-50) :: 18mg/ jour
- Grossesse :: les besoins s’élèvent à 27mg/ jour. *Allaitement :: 9mg/ jour
La limite maximale se situe à 45mg/ jour pour tous SAUF les enfants, pour qui le plafond est à 40mg/ jour.
Toute dose allant au-delà de ces valeurs de références devrait être évaluées et suivie par un professionnel de santé.
Voilà!
Ces chiffres représentent les apports qui devraient couvrir les besoins de la majorité des individus sains.
Bien que suffisant pour la majorité, ces approximations ne sont pas nécessairement optimales pour tous. L’individualisation de ces suggestions devraient être considérée; la lecture du texte plus bas vous aidera à évaluer vos besoins potentiels. Pas envie de lire?! Un naturopathe vous sauvera le blabla et saura vous guider à travers l’info qui vous est pertinente. 😉
English version here.
Le Fer :: ce que c’est et ce que ça fait
Le fer est un minéral que l’organisme ne peut PAS fabriquer et qui est essentiel à sa croissance, son entretien et ses diverses fonctions.
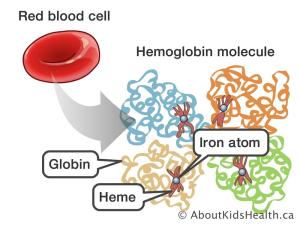
- C’est un composé fondamental de l’hémoglobine (et de la myoglobine); elle-même une structure vitale des globules rouges qui transportent l’oxygène à travers nos systèmes. Le fer est également utile à la production d’énergie (cytochrome C de la chaine respiratoire).
- Il est un cofacteur majeur dans l’assemblage de certains enzymes et dans la stabilisation de certaines protéines (via protéines Fer-Soufre). *Les enzymes (des protéines!) sont ESSENTIELLES au fonctionnement de notre constitution :: sans elles les réactions biochimiques sont trop longues et lentes et la vie n’est plus possible.
- En tant que constituant de la superfamille d’enzymes “Cytochrome P450”, le fer contribue à la régulation/ dégradation des xénobiotiques (pollution, plastiques et parfums), des acides gras et d’autres composés variés. Le CYP450 est également impliqué dans la production et la dégradation de différentes hormones. La production de TSH et la conversion de la T4 en T3 en sont 2 exemples (lire :: santé de la thyroïde!). Les cytochromes de cette famille jouent également un rôle dans la régulation des surrénales (on pense :: stress et vigilance!), le métabolisme de l’insuline (on retient :: énergie stable!), régulation des hormones sexuelles (via conversion des androgènes en œstrogènes, par exemple), reconnaissance de dommages et réparation de l’ADN1, 2, 3, 4 …
- Les taux de fer circulant ont aussi un impact important sur la leptine, hormone de satiété. Les individus souffrant d’anémie ressentent fréquemment une perte d’appétit due à un fer inadéquat lui-même incsuffisant pour faire DIMINUER la leptine circulante. La supplémentation en fer, ou son apport alimentaire suffisant, engendre un effet inhibiteur de la leptine-j’ai-pas-faim. Cet effet « suppresseur de leptine/ suppresseur de satiété » a pour but d’AUGMENTER l’appétit afin que l’individu puisse profiter de l’abondance en fer alimentaire perçue, et refasse le plein 5 .
- Fe2+, Ferreux // fer HÉMinique :: principalement de sources animales
- Fe3+, Ferrique // fer NON-HÉMinique :: de sources végétales
Les différents mécanismes d’absorption reliés à ces 2 formes distinctes sont présentés ici.
En version courte ::
- Le fer d’origine animale est MOINS abondant dans la diète moyenne et aisément absorbé
- Le fer d’origine végétale est PLUS abondant dans la diète moyenne mais n’est pas aussi bien absorbé
La consommation et supplémentation en fer devrait être approchée avec prudence puisque ce nutriment est à la fois ESSENTIEL au bien-être et DÉLÉTÈRE lorsque consommé en excès.
La sursaturation en fer de l’organisme déclenche la production de radicaux libres qui cause le vieillissement prématuré et accéléré de nos cellules.
Une image que j’aime garder en tête est celle du « fer qui rouille ». Bien que pas 100% juste ou exacte, je trouve que cette analogie est un bon rappel de ce qui peut se produire à l’interne quand la régulation du fer tourne mal et que le métal s’accumule et devient réactif.
Sources principales
Sources de fer d’origine animale::
- Bœuf (faux-filet) :: 100 g – 2.9mg *Voir aussi :: foie
- Huîtres (crues) :: 100 – 5.1mg *Voir aussi :: pieuvre, moules et seiche
- Thon (conserve) :: 100g – 1.5mg *Voir aussi :: sardines
- Poulet (poitrine, sans peau) :: 100g – 1.1mg
- Porc (haché, cuit) :: 100g – 1.3mg
Sources de fer d’origine végétale ::
- Abricots séchés :: 100g – 2.7mg *Voir aussi :: pruneaux, figues séchées et raisins secs
- Lentilles :: 100g – 3.3mg *Voir aussi toutes les légumineuse, tofu et tempeh
- Épinards (crus):: 100g – 2.7mg *Voir aussi :: bette à carde et brocoli
- Épinards (cuits):: 100g – 3.6mg
- Chocolat à cuisson, non sucré:: 100g – 17.4mg *Voir aussi :: poudre de cacao
- Flocons d’avoine (secs, grains entiers) :: 100g – 4mg *Voir aussi :: quinoa et orge
- Pleurotes (crus) :: 100g – 1.3mg
- Graines de citrouille :: 100g – 8.1mg *Voir aussi graines de sésame
**Quelques produits tels céréales, nouilles, pains et bagels, bien qu’ils ne représentent habituellement PAS une source significative de fer, sont maintenant enrichis/ fortifiés avec du fer.
Un organisme sain est tout à fait capable de réguler l’absorption du fer en fonction de ses besoins; la “surdose” ALIMENTAIRE est extrêmement rare.
Des problèmes peuvent par contre se présenter avec la SUPPLÉMENTATION, renforçant l’idée que la correction et l’optimisation de l’alimentation devrait toujours être le premier réflexe pour la majorité d’entre nous.
La consommation excessive de fer est liée à un stress oxydatif accru.
Évaluation des besoins en fer
- Diète végétarienne et consommation quotidienne de légumineuses et légumes feuilles vert foncé 6 :: pas très fan de l’un ou l’autre? Ces 2 riches sources de fer ne se retrouvent pas souvent au menu? Il serait judicieux de faire évaluer vos taux et/ou vos apports.
- Les gens consommant une diète de “pseudo aliments” pauvres en nutriments sont à risque de ne pas satisfaire leurs besoins en fer (et autres!).
- La grossesse fait augmenter les besoins moyens de 9mg :: connaissez-vous la quantité de fer que vous consommer au quotidien? Seriez-vous en mesure de créer un repas ou une collation totalisant 9mg? Si la réponse est non, un suivi en naturopathie pourrait vous être utile.
- Menstruations :: il y a une évaluation à faire ici. Légères? Courtes? Longues? Abondantes? Toute combinaison de ces 4 descriptifs aura un impact distinct sur les besoins.
- Les besoins des athlètes de haut niveau sont toujours considérés comme un peu plus haut que la moyenne (hémolyse, sudation excessive…). *Les adeptes de santé physique/ gym n’ont pas à s’en faire; la majorité d’entre nous ne voyons pas nos besoins accroitre parce qu’on bouge 1h… ou 2… ou 3 par jour! 😉
- Les saignements chroniques engendrés par diverses pathologies :: ulcères gastriques, polypes intestinaux, cancer du côlon, maladie Cœliaque… L’endométriose peut aussi provoquer des saignements dont on peut ne PAS être conscient. Tout type de saignement récurrent pourrait suggérer des besoins en fer accru.
- Ingestion fréquente d’aspirine :: agent irritant de la muqueuse gastrique notoire, des saignements pourraient être présent à votre insu.
- Pontage gastrique :: le processus digestif n’étant plus complet, ni optimal, il est impératif de respecter la fréquence des suivis médicaux établit par votre médecin traitant. Un naturopathe peut quant à lui vous accompagner dans l’optimisation de votre nouvelle condition digestive.
- Maladies infectieuses et inflammatoires (inclut l’obésité!) jouent également des rôles déterminant dans l’évaluation des besoins. Ceux-ci pourraient être légèrement plus élevé que la moyenne 7.
Optimiser l’absorption
Le poivre noir est une de ces substances largement reconnue comme “potentialisatrice d’absorption“. Certaines études corrèlent la Bioperine*/ pipérine avec une meilleure absoprtion du fer 8 .
*Bioperine est le nom commercial d’un type d’extrait de pipérine de poivre noir.
La consommation d’algues peut aussi être un choix judicieux lorsqu’une absorption de fer accrue est souhaitée. “La biodisponibilité de ce fer (algal) semble être élevée et, accroit par 5X l’absorption apparente du fer d’un repas de riz seul. Ce phénomène est probablement attribuable à sa forte concentration en vitamine C et son contenu en phytates faible voir, non existant. 9”
Bien qu’il y ait PLUSIEURS sources entières de végétaux marins à notre disposition, la consommation d’algues en Amérique du Nord reste faible. L’ajout de dulse ciselée (BACON de mer!) sur une salade, une petite poignée de wakame réhydratée dans un plat de nouilles à saveur asiatique, une classique feuille de nori enroulée autour de morceaux d’avocats, de gingembre mariné et de riz brun; il y a mille et une façons d’intégrer quotidiennement ces petites bombes minérales à notre alimentation.
Si la supplémentation s’avérait nécessaire, après évaluation professionnelle, la prise de suppléments pourrait être faite tous les 2 jours afin de maximiser l’absorption.
Voici pourquoi ::
Quand le fer est 1-présent, et 2-absorbé, il engendre une sécrétion de l’hormone régulatrice du fer, l’hepcidine. En somme, quand le fer est abondant, l’hepcidine s’ÉLÈVE de manière à raaaalentiir son absorption. Elle prévient les surcharges qui pourraient être causées par une absorption non régulée (Ex. :: hémochromatose).
Une étude de 2020 (sur 19 femmes) suggère que la prise de suppléments de fer en jour alternés (1 jour sur 2) offre une pause nécessaire à la diminution de l’hepcidine. Ce qui veut dire :: moins d’hepcidine = + d’absorption de fer! Cette petite altération toute simple à la posologie aurait le pouvoir de bien rentabiliser vos dollars et de maximiser vos efforts de reconstitutions de stocks de fer. 10, 11, 12 .
La vitamine C est un cofacteur classique bonifiant l’absorption du fer végétal 13 .
Joueurs importants // Alliés du fer
B6 – Pyridoxine :: Cette vitamine hydrosoluble est essentielle à la formation de globule rouge (érythropoïèse) Elle joue un rôle fondamental dans l’incorporation du fer à l’hème de notre HÉMoglobine (protoporphyrine). Des apports sous optimaux de cette vitamine sont liés à une incidence d’anémie accrue et plusieurs autres problèmes de santé 15, 16 .
B9 – Folate :: celle-ci travaille également (conjointement avec le fer, la B6 et la B12) à la bonne formation de globules rouges. L’absence de l’une ou l’autre de ces molécules, dans l’élaboration d’une cellule sanguine de qualité, en revient à tenter de voyager sans passeport, ni billet. L’abondante consommation d’alcool, la maladie cœliaque et le syndrome du côlon irritable augmentent TOUS les besoins en B9 17, 18, 19.
B12 – Cobalamine :: Cette vitamine joue un rôle important dans la prolifération cellulaire. Les globules rouges ayant une durée de vie utile d’environ 120jours; leur renouvellement est constant. Avec la B6 et la B9, la B12 assure la croissance adéquate des érythrocytes. Une cellule sanguine déficiente en B12 est non conforme et donc inefficace; elle est dégradée avant de pouvoir faire son travail. La cobalamine impact donc le fer de manière indirecte en assurant l’intégrité des globules rouges qui elles, garderont l’hémoglobine (et le fer!) dans le compartiment cellulaire ainsi prévenant un « besoin perçu » de fer que le corps chercherait à pallier A.
Cuivre :: ce minéral est nécessaire au transport et au « dispatch » du fer. Comme le fer, une approche « à la Boucle d’Or » est à mettre en place quand on veut optimiser ses niveaux; trop peu ou trop TROP auront tous 2 des effets délétères sur le bien-être 20, 21. La supplémentation sans l’avis d’un professionnel est déconseillée.
Les principales sources alimentaires de cuivre sont les suivantes :: foie, chocolat noir, huitres, légumes feuilles vert foncé, spiruline, noix & graines et champignons shiitake. Si le rôle exact du cuivre dans le métabolisme du fer vous intéresse, lisez cet article sur le métabolisme du fer.
Précautions
Les inconforts liés à la supplémentation en fer les plus commun touchent la sphère gastro-intestinale.
Encore une fois, ces inconforts désagréables sont une autre bonne raison de privilégier les sources alimentaires plutôt que les capsules dans les cas où c’est possible.
Douleurs gastriques, nausée, vomissements, alternance constipation & diarrhée sont les principaux coupables. Les suppléments de fer sont mieux absorbé sur un estomac vide; mais encore faut-il qu’il soient tolérés!? La plupart des gens préfèreront le prendre avec une petite quantité de nourriture pour adoucir les inconforts qui y sont liés.
La supplémentation sur journées alternées, telle que suggérée plus tôt pour bonifier l’absorption, tend aussi à réduire les risques de manifestations désagréables ET augmenter l’adhésion au protocole de supplémentation.
Apports exagérés
Fer et Cancer du sein :: une diète PAUVRE en antioxydants et abondante en gras et en fer pourrait faire augmenter l’incidence de cancer du sein (via peroxydation lipidique) 22.
Fer et Infarctus du myocarde :: la surconsommation de fer HÉMINIQUE, de sources animales, couplée à une diète pauvre en minéraux responsable de DIMINUER l’absorption du fer peut mener à des troubles cardiovasculaires 23 .
Fer et Diabète de Type 2 :: encore, la surconsommation de fer HÉMINIQUE, de sources animales, peut mener à une risque accru de développer le diabète de type 2 24 .
Fer et Cancer colorectal :: encore une fois, tous ensemble :: la SURconsommation de fer (tous types) ou un protocole de supplémentation mal évalué pourrait mener à un risque accru de développer le cancer colorectal 25 .
Apports sous-optimaux et risques associés
Un des désordres les plus communs lié au fer est l’anémie. Celle-ci prend plusieurs formes. J’écrirai un article sur le sujet bientôt.
Apprenez à reconnaitre les signes classiques pouvant être associés à des taux de fer inadéquats et consultez votre médecin de famille si vous avez des inquiétudes.
- Fatigue intense – Même après le repos
- Souffle court
- Douleur à la langue
- Rythme cardiaque irrégulier
- Faiblesse
- Douleur à la poitrine
- Étourdissements // Vertiges
- Extrémités froides
- Ongles fragiles
- Pâleur de la peau
- Maux de tête
Facteurs moins connus qui pourraient influencer les besoins
La prise d’Inhibiteurs de Pompe à Proton, tel que l’omeprazole, pour traiter la détresse gastro-œsophagienne et/ou prévenir les ulcères gastriques causés par une prise régulière d’aspirine ou autres anti-inflammatoires non-stéroïdiens élève le risque de carence en fer 26 .
La consommation régulière, et à dose importante, de suppléments de quercétine est suspectée de faire augmenter la sécrétion d’hepcidine qui elle, DIMINUE l’absorption du fer. La supplémentation de quercétine semble aussi réduire le nombre disponibles de transporteurs intestinaux en charge de l’absorption du fer végétal et donc, influence l’absorption à la baisse (DMT1). La quercétine est souvent suggérée, entre autres, pour soutenir les états allergiques.
*L’envers de la médaille :: si un individu se trouve en situation de “surabondance” de fer dans l’organisme, la quercétine peut s’avérer être une avenue efficace de minimisation de l’absorption de minéral. Une discussion avec votre professionnel de la santé est un point de départ impératif en ce cas 27 .
Avez-vous des “rages/ envies” de substances non-alimentaires/ non-nutritives comme la terre, la glace, le caoutchouc ou l’argile? Cette condition se nomme « Pica » et peut être un indicateur de taux de fer insuffisant 29 .
Une perte de cheveux soudaine et/ou soutenue et inexpliquée? Bien que le mécanisme impliquant le fer dans la croissance et la rétention capillaire ne soit pas tout à fait clair; il y a une corrélation largement accepté comme signe additionnel pouvant indiquer un apport en fer insuffisant 30, 31 .
Le syndrome des jambes sans repos (Restless legs syndrome) fait un peu le même cas de figure que la perte de cheveux; bien que mal expliqué, la corrélation de ce phénomène à des taux de fer inadéquats est significative 32, 33.
Troubles de comportements et/ou difficultés d’apprentissage, SURTOUT durant l’enfance et l’adolescence. Certains décrivent des manifestations s’apparentant au « TDAH ». Ce « symptôme » est plutôt vague et DOIT définitivement être évalué par un professionnel de santé; l’auto-perception de déficit est un indicateur important indiquant qu’une discussion DOIT être entamée avec votre/ vos professionnels de santé. Un million de facteurs peuvent influencer le comportement et la cognition humaine; un apport en fer sous-optimal n’en est qu’un parmi tant d’autres 34.
Toujours se rappeler :: Aucun “signe ou symptôme” isolé ne représente une carence en fer inadéquat à lui seul. TOUS les facteurs doivent être cumulés et analysés avec une approche, un mentalité, multifactorielle.
Tests Sanguins
*Les tests sanguins sont prescrits et interprétés par un docteur en médecine. Les valeurs caractérisant l’abondance du fer dans l’organisme peuvent être ajoutées à tout bilan sanguin; vous n’avez qu’à demander.
Valeurs de Référence
Elles diffèrent selon les sexes et sont plutôt nombreuses quand vient le temps d’évaluer l’effet d’ensemble des taux de fer sur la biochimie. Ici se trouve un lien menant à des valeurs approuvées par le corps médical Canadien pour ceux qui sont curieux.
Les valeurs sanguines sont impératives dans l’évaluation des besoins d’un individu. D’autres aspects de la santé globale doivent également être pris en compte durant l’analyse des résultats afin de soutenir la vitalité de façon judicieuse et vraiment personnalisée.
Quelques combos inhibant possiblement l’absorption
Aliments et combinaisons à éviter, 2hrs avant et 2hrs après une dose thérapeutique ou un repas intentionnellement riche en fer visant à faire augmenter les taux 35, 36 ::
- Les polyphénols/ aliments riches en tanins :: thé, café, vin et chocolat noir, entre autres, ont un effet astringent/ “resserrant” sur les muqueuses digestives et rendent l’absorption de certains nutriments, pas seulement le fer, un peu moins efficace. L’effet des aliments riches en tanins/ polyphénols est proportionnel à la dose; plus la quantité consommée est grande, plus l’effet inhibiteur d’absorption est important. Une consommation minimale peut être contrée par l’ajout régulier de sources de vitamine C à la diète 37 .
- Les aliments riches en acide phytique comme les grains, les légumineuses, noix & graines CRUES. Comme pour les polyphénols, l’effet des phytates est “dépendant de la dose” ingérée. La cuisson, la fermentation, le germination et le trempage contribuent TOUS à diminuer le contenu en acide phytique des aliments qui en contiennent. Puisque la plupart des aliments listés dans cette catégorie se consomment très peu crus, ils ne sont au final que sources négligeables d’anti-nutriments. *Pour les noix et les graines, un trempage de 8hrs (Ex. :: durant la nuit, puis rincées et réfrigérées) ou l’achat de produits « Crus & Activés » où le trempage et le séchage a été fait pour vous sont d’excellentes alternatives à considérer quand la remontée des taux de fer est visée et/ou que les sources d’acide phytique doivent être diminuées.
(*Malentendu commun :: l’acide oxalique/ les oxalates ne sont PAS des phytates/ acides phytique. Ils sont une « bête » complètement différente et n’ont pas d’effet inhibiteur sur l’absorption du fer.)
- Aliments riches en calcium :: fortement identifiés comme inhibiteur d’absorption du fer dans le passé, la corrélation n’est maintenant plus si tranchante.
Si vous êtes sous supplémentation thérapeutique, il serait probablement judicieux d’éviter de supplémenter ces 2 minéraux simultanément. Mais sous forme d’aliments entiers faisant partie d’une diète bien planifiée ne visant pas à pallier des apports déficients, je vous invite à ne pas vous casser la tête avec cette interaction. Elle est en général de courte durée EEETTT est compensée par une augmentation des transporteurs (absorbeurs!) de fer quelques heures après l’ingestion de sources de calcium concentrées.
- Les protéines d’œufs :: elles auraient un effet inhibiteur sur l’absorption du fer ET le fer que les œufs contiennent, une fois cuit, est de faible biodisponibilité. *Œufs à la coque/ cuit durs :: quand le jaune tourne un peu grisâtre/ verdâtre? On parle de sulfure de fer/ sulfure ferreux –> absorbabilité très limitée.
- Antiacides 38
- Antibiotiques et certains autres médicaments :: Les suppléments de fer peuvent diminuer l’absorption de certains médicaments et les rendre MOINS efficaces. Aussi, certains médicaments peuvent augmenter l’absorption et le stockage du fer à des niveaux inquiétants. La règle du 2hrs avant/ 2 hrs après est très pertinente ici, à moins d’avoir le feu vert du médecin traitant. Quelques interactions sont listées dans cet article.
- Le curcuma –> controversé :: certaines études suggèrent que le curcuma aurait un effet stimulant sur l’absorption du fer via un mécanisme anti-inflammatoire répresseur de l’hepcidine39. MAIS, certaines études effectuées avec des doses de curcuma élevées lui attribuent des propriétés chélatrices inhibitrices de l’absorption du fer 40. Une évaluation individuelle des apports et des besoins en ces 2 substances est logiquement requise dans ce cas-ci.
AUSSI :: si vous suivez un protocole impliquant des compléments de fer; éviter de consommer des aliments fortifiés en fer de manière à limiter la SURconsommation de ce minéral. *A moins que le professionnel traitant n’ait intégrer l’apport de certains de ces aliments dans son approche thérapeutique.
Voici qui conclut la fiche du Fer!
Quelques études sont intégrées à même cet article, n’hésitez pas à lire plus en profondeur sur le sujet; ce billet n’est qu’une synthèse rapide et simplifiée du sujet.
Si besoin il y a, envoyez ou présentez certaines études à votre praticien de santé afin d’évaluer ensemble si votre condition permet des taux de fer compatibles avec le niveau de bien-être que vous recherchez.
Restez humble et curieux,
Soyez bien,
Vicky x
Vicky Bachand ND.A est naturopathe :: un naturopathe ne remplace PAS un médecin.
Les renseignements contenus dans cet article sont présentés strictement à titre informatif et ne visent pas à fournir des renseignements complets sur les sujets traités ni à remplacer les conseils d’un professionnel de la santé qualifié.
Ces renseignements ne constituent ni une consultation, ni un diagnostic ou une opinion médicale, et par conséquent, ne doivent pas être interprétés comme tels.
Consulter toujours votre professionnel de la santé si vous avez des questions au sujet de votre état de santé.